The medical field has long been enriched by the contributions of pioneering figures whose innovations continue to shape contemporary practice. Among these lasting contributions is a technique developed in the Victorian era that remains relevant for the assessment and management of conditions affecting the ear. Named after Joseph Toynbee, a prominent figure in the history of otology, this simple yet effective procedure has withstood the test of time and continues to feature in modern audiology and otolaryngology settings. Understanding the Toynbee manoeuvre requires not only a grasp of its clinical mechanics but also an appreciation of the historical context in which it emerged. This article explores the origins, underlying physiology, practical applications, and ongoing significance of this enduring medical technique.
Historical Origins and Development of the Toynbee Manoeuvre
Joseph Toynbee and the Birth of Otological Innovation
The emergence of the Toynbee manoeuvre is intimately connected to the broader evolution of otorhinolaryngology during the nineteenth century, a period marked by remarkable advances in the understanding of ear anatomy and physiology. Joseph Toynbee, an English physician born in the early 1800s, dedicated much of his career to the study of otology and was instrumental in expanding the knowledge of middle ear dysfunction. His work was part of a wider movement in European medicine that sought to systematically examine the relationship between anatomical structures and hearing loss. Toynbee introduced several innovations, including the otoscope in 1850, which allowed clinicians to visualise the eardrum and middle ear structures more effectively. His contributions were built upon the foundations laid by earlier researchers, including Edm Gilles Guyot, who in 1724 first described Eustachian tube catheterisation, and Archibald Cleland, who in 1741 published a method of catheterisation through the nose. These pioneering efforts reflected a growing interest in the Eustachian tube and its critical role in regulating middle ear pressure, a concept that Nicolas Deleau the Younger would later explore in the 1820s and 1830s. Deleau recognised the importance of the Eustachian tube in maintaining normal hearing and classified the different noises heard during catheterisation procedures, thereby advancing diagnostic techniques in otology.
Evolution of the Technique Through Medical Literature
As the nineteenth century progressed, the medical community increasingly appreciated the importance of pressure equalisation in the middle ear. The technique that would come to bear Toynbee's name emerged from this evolving understanding. By the mid-1800s, clinicians had begun to refine methods for assessing Eustachian tube function, driven by the recognition that obstruction of this passage could lead to a range of symptoms including earache, fullness, tinnitus, and dizziness. The development of the Toynbee manoeuvre was part of a broader effort to provide practitioners with simple, non-invasive tools for evaluating and treating middle ear conditions. During this period, the work of figures such as Laennec, who in 1825 used a stethoscope to assess Eustachian tube patency, and Hubert-Valleroux, who in 1843 questioned the necessity of artificial eardrum perforation, contributed to a more nuanced approach to managing ear disorders. The integration of the Toynbee manoeuvre into clinical practice reflected a shift away from invasive procedures towards more conservative diagnostic and therapeutic strategies. This evolution was further supported by the anatomical insights of the Renaissance, when figures like Leonardo da Vinci provided detailed descriptions of the nasal conchae and paranasal sinuses in 1489, and by the detailed observations of Alfonso Corti, who described the Organ of Corti, the true site for hearing, in the nineteenth century. These historical milestones collectively underscored the importance of understanding the intricate connections between the ear, nose, and throat, a principle that continues to inform modern ENT medicine.
The physiological mechanism behind the toynbee manoeuvre
Understanding eustachian tube function and pressure equalisation
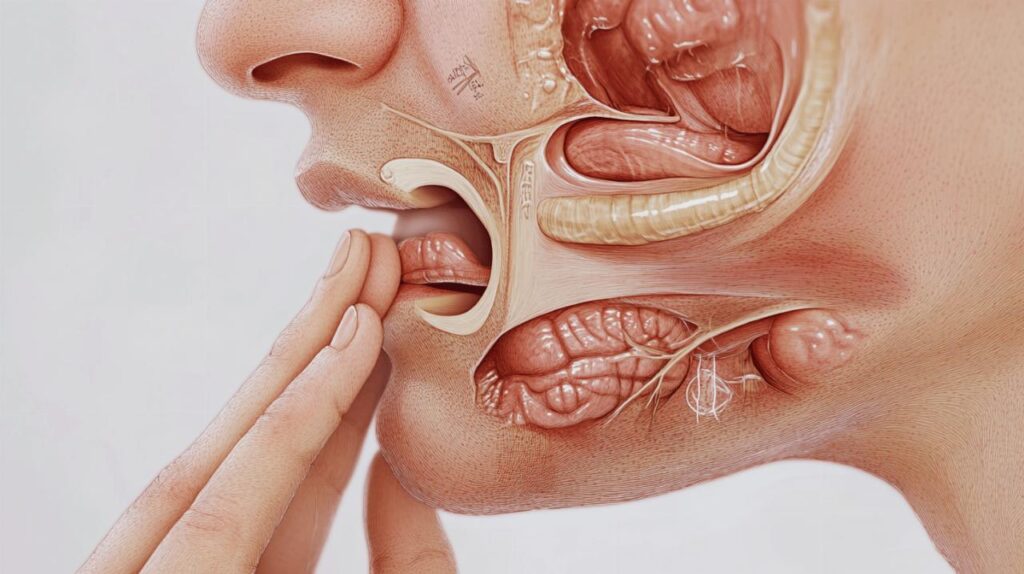
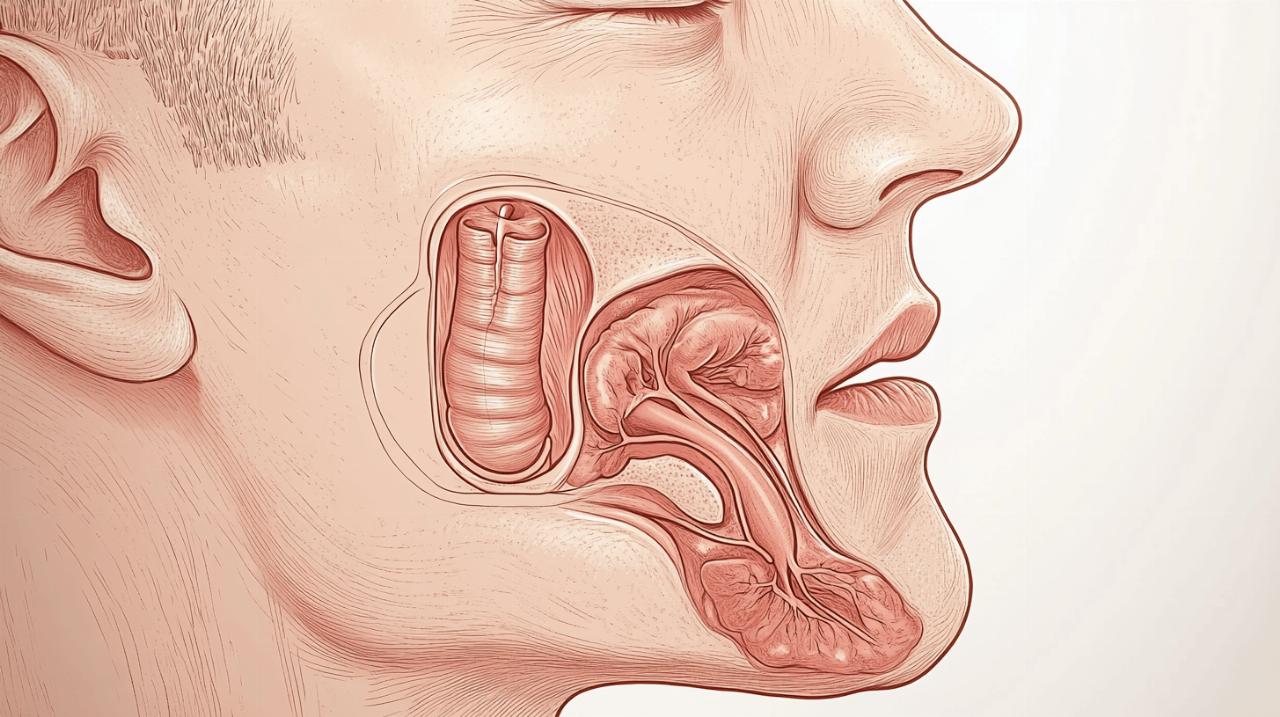
To appreciate the Toynbee manoeuvre, one must first understand the fundamental role of the Eustachian tube in maintaining auditory health. This narrow passage, which connects the middle ear to the nasopharynx, is responsible for equalising pressure on either side of the eardrum. Under normal circumstances, the Eustachian tube remains closed but opens briefly during swallowing, yawning, or other movements of the jaw and throat. This opening allows air to enter or exit the middle ear, ensuring that the pressure within this cavity matches atmospheric pressure. When the Eustachian tube becomes obstructed or fails to function properly, a pressure imbalance can develop, leading to discomfort, impaired hearing, and in some cases, more serious complications such as middle ear effusion or infection. The Toynbee manoeuvre exploits the natural physiology of swallowing to assess the patency and function of the Eustachian tube. By creating a negative pressure within the nasopharynx through a combination of swallowing and nasal occlusion, the technique encourages the Eustachian tube to open, thereby facilitating the equalisation of middle ear pressure. This mechanism is closely related to other physiological processes that were explored during the nineteenth century, a time when researchers were beginning to unravel the complexities of auditory physiology and the vestibular system. The work of Nobel Prize laureate Robert Barany in 1914, who received recognition for his contributions to the understanding of the physiology and pathology of the vestibular system, exemplifies the broader scientific curiosity that characterised this era. The Toynbee manoeuvre thus represents a practical application of these physiological principles, offering clinicians a straightforward means of evaluating Eustachian tube function without the need for invasive procedures.
Step-by-Step Breakdown of the Swallowing Technique
The execution of the Toynbee manoeuvre is relatively simple, yet it requires careful attention to technique in order to achieve reliable results. The procedure begins with the patient closing their mouth and pinching their nostrils shut to create a sealed environment within the nasopharynx. With the nostrils occluded, the patient is then instructed to swallow. The act of swallowing initiates a sequence of muscular contractions that ordinarily facilitate the opening of the Eustachian tube. However, because the nostrils are closed, the swallowing action creates a negative pressure within the nasopharynx and, by extension, within the middle ear. This negative pressure can be detected using various diagnostic tools, such as tympanometry, which measures changes in the compliance of the eardrum in response to pressure variations. The resulting movement of the tympanic membrane provides valuable information about the patency and function of the Eustachian tube. In clinical practice, the Toynbee manoeuvre is often performed in conjunction with other tests to provide a comprehensive assessment of middle ear function. The simplicity of the procedure makes it particularly valuable in settings where more sophisticated diagnostic equipment may not be readily available. Moreover, the technique can be easily taught to patients, allowing them to perform it at home as part of a self-management strategy for conditions such as barotrauma or Eustachian tube dysfunction. The ability to perform the manoeuvre without specialised instruments or invasive intervention underscores its enduring relevance in modern medical practice, a testament to the ingenuity of its nineteenth-century origins.
Clinical applications and modern medical practice
Diagnostic Uses in Audiology and Otolaryngology
The Toynbee manoeuvre has found widespread application in both audiology and otolaryngology, where it serves as a valuable diagnostic tool for assessing Eustachian tube function. In audiology clinics, the manoeuvre is frequently employed during tympanometry, a procedure that measures the mobility of the eardrum in response to changes in air pressure. By performing the Toynbee manoeuvre while tympanometry is being conducted, clinicians can observe how the Eustachian tube responds to the negative pressure created by swallowing with occluded nostrils. This information is crucial for diagnosing conditions such as Eustachian tube dysfunction, which can manifest as a sensation of fullness in the ear, hearing loss, or recurrent middle ear infections. In otolaryngology, the manoeuvre is often used as part of a broader assessment of patients presenting with symptoms related to middle ear pressure imbalance. The technique is particularly useful in evaluating patients who have undergone nasal surgery or who suffer from conditions affecting the paranasal sinuses, as these factors can influence Eustachian tube function. The historical evolution of endoscopic surgery, including the development of functional endoscopic sinus surgery and the trans-sphenoidal approach pioneered by Harvey Cushing in 1912, has provided clinicians with enhanced visualisation and understanding of the anatomical structures involved. The integration of modern imaging techniques, such as CT scans, has further refined the diagnostic process, allowing for a more comprehensive evaluation of the ear, nose, and throat. The Toynbee manoeuvre, with its roots in nineteenth-century medical innovation, continues to complement these advanced technologies by offering a simple, cost-effective means of assessing Eustachian tube patency.
Treatment Protocols for Middle Ear Dysfunction and Barotrauma
Beyond its diagnostic applications, the Toynbee manoeuvre plays an important role in the treatment of various middle ear disorders. One of the most common clinical scenarios in which the manoeuvre is employed is the management of barotrauma, a condition that occurs when rapid changes in atmospheric pressure lead to a disparity between the pressure in the middle ear and the external environment. Barotrauma is frequently encountered in situations such as air travel, scuba diving, or even rapid changes in altitude during driving. The Toynbee manoeuvre offers a non-invasive method for patients to alleviate the discomfort associated with barotrauma by facilitating the equalisation of middle ear pressure. In addition to its use in acute situations, the manoeuvre is incorporated into treatment protocols for chronic Eustachian tube dysfunction, a condition that can significantly impair quality of life. Patients with chronic dysfunction are often taught to perform the manoeuvre regularly as part of a self-management regimen. This approach reflects a broader trend in modern medicine towards empowering patients with tools and techniques that enable them to take an active role in managing their health. The development of hearing prostheses and cochlear implants, which have revolutionised the treatment of hearing loss since their introduction in the twentieth century, underscores the importance of ongoing innovation in otology. However, the Toynbee manoeuvre remains a cornerstone of conservative management, particularly in cases where more invasive interventions are not warranted. The historical context in which the manoeuvre was developed, an era marked by significant advances in local anaesthesia, microscopic surgery, and the understanding of cholesteatoma and mastoiditis, highlights the enduring value of simple, patient-centred techniques in the broader landscape of ENT medicine.
Practical guidelines and patient considerations
Performing the Toynbee Manoeuvre Safely and Effectively
For patients and clinicians alike, understanding the proper technique for performing the Toynbee manoeuvre is essential to ensuring its effectiveness and safety. The procedure should be conducted in a calm and controlled manner, with clear instructions provided to the patient. It is important that the patient fully understands the need to pinch their nostrils closed before swallowing, as failure to create an adequate seal can compromise the reliability of the test. Once the nostrils are occluded, the patient should swallow gently, avoiding excessive force, which could potentially cause discomfort or adverse effects. In clinical settings, the manoeuvre is typically performed under the supervision of a trained professional who can monitor the patient's response and provide immediate feedback. The use of tympanometry or otoscopy during the procedure allows the clinician to objectively assess the movement of the eardrum and the patency of the Eustachian tube. For patients who are instructed to perform the manoeuvre at home, it is advisable to practice the technique initially in the presence of a healthcare provider to ensure correct execution. The simplicity of the manoeuvre makes it accessible to a wide range of patients, including children and the elderly, although care must be taken to adapt the instructions to suit the patient's level of understanding. The historical development of the otoscope by Joseph Toynbee in 1850 revolutionised the visualisation of the ear and remains a fundamental tool in the assessment of middle ear function. Similarly, the Toynbee manoeuvre exemplifies the practical application of anatomical and physiological knowledge in a manner that is both straightforward and effective. Patients who experience difficulty performing the manoeuvre or who do not achieve the desired relief should be encouraged to consult their healthcare provider for further evaluation and alternative management strategies.
Contraindications, limitations and alternative manoeuvres
While the Toynbee manoeuvre is generally considered safe and well-tolerated, there are certain contraindications and limitations that must be taken into account. Patients with acute ear infections, perforated eardrums, or recent ear surgery should avoid performing the manoeuvre without first consulting their healthcare provider, as the changes in pressure could exacerbate these conditions or lead to complications. Additionally, individuals with severe nasal congestion or anatomical abnormalities affecting the Eustachian tube may find the manoeuvre less effective, as the underlying obstruction can prevent the proper equalisation of middle ear pressure. In such cases, alternative manoeuvres, such as the Valsalva manoeuvre, may be recommended. The Valsalva manoeuvre involves exhaling forcefully against a closed airway, which increases pressure in the nasopharynx and can help to open the Eustachian tube. However, this technique carries a higher risk of causing barotrauma if performed incorrectly, and it is generally considered less gentle than the Toynbee manoeuvre. The choice of technique should be guided by the patient's specific clinical situation and the judgement of the healthcare provider. The historical evolution of otorhinolaryngology, from the ancient treatments described by Egyptians, Greeks, and Hindus, through the Renaissance anatomy of Leonardo da Vinci and Michelangelo, to the modern era of antibiotics, radiotherapy, and advanced surgical techniques, has provided a rich tapestry of knowledge and practice. The introduction of optic fibre endoscopes by Karl Storz in 1954 and the subsequent development of functional endoscopic sinus surgery have further expanded the diagnostic and therapeutic options available to clinicians. The Toynbee manoeuvre, with its roots in the nineteenth century, continues to hold a place in this evolving landscape by offering a safe, effective, and accessible means of managing middle ear pressure disorders. As medical knowledge and technology continue to advance, the principles underlying the manoeuvre remain as relevant today as they were over a century ago, a testament to the enduring legacy of Joseph Toynbee and his contributions to the field of otology.




